Table of Contents

She walked into my center gripping her right shoulder, convinced it was frozen. Three clinics, two rounds of physical therapy, and still no relief. But the moment I watched her breathe, I understood the real problem had nothing to do with her shoulder at all. This is the story I see repeated every single week — and it is why diaphragm and shoulder pain remains one of the most misunderstood connections in the human body.
Most people treat shoulder pain as a local problem. They stretch the rotator cuff, apply heat, visit massage therapists, and wonder why the tension always returns. What they do not realize is that diaphragm and shoulder pain share a neurological and mechanical relationship that runs far deeper than surface-level muscle tension. Until that root connection is addressed, no amount of shoulder-focused treatment will produce lasting relief.
The Anatomical Link You Were Never Told About
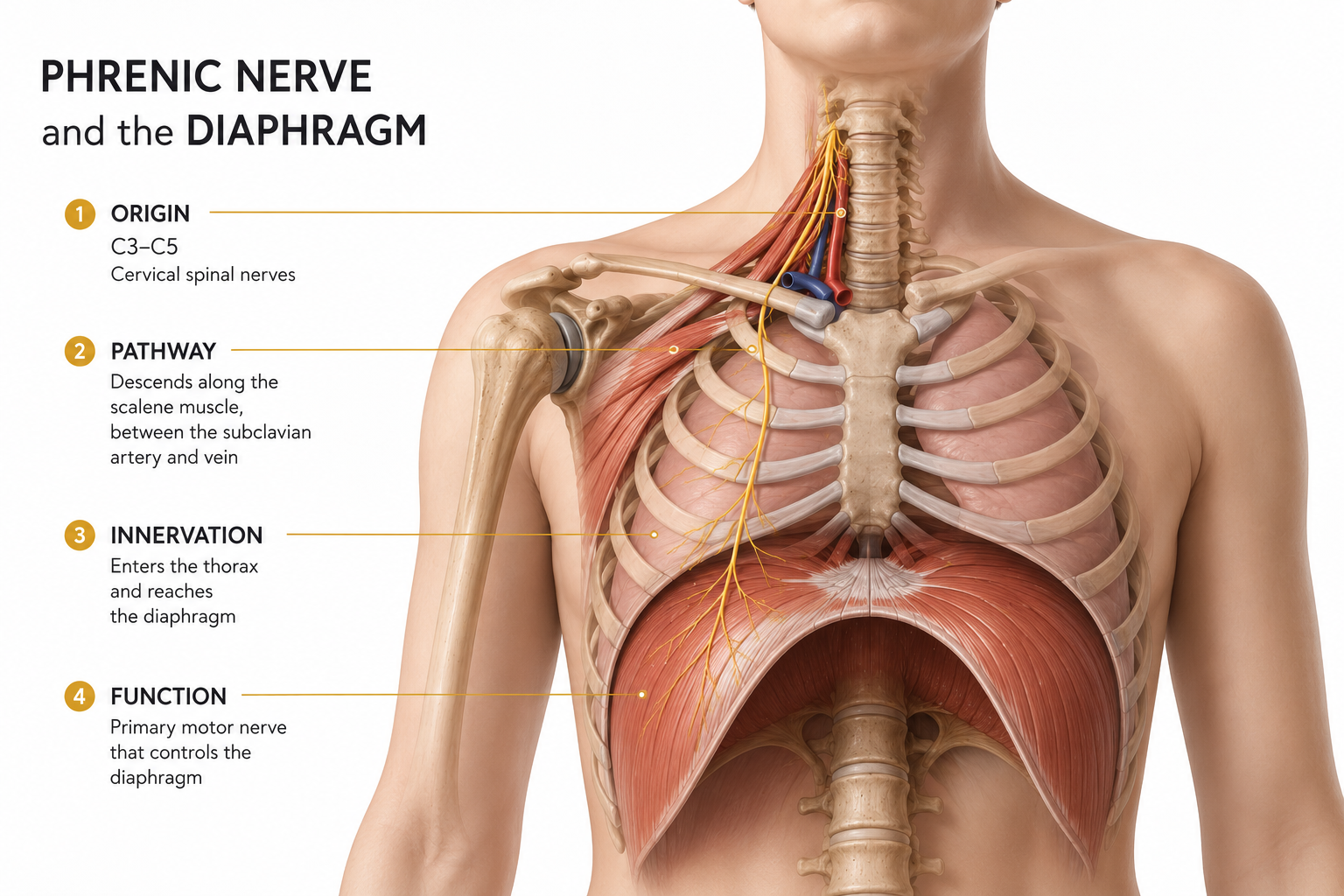
The diaphragm is your primary breathing muscle — a dome-shaped structure separating your chest cavity from your abdomen. What most people never learn is that the phrenic nerve, which controls the diaphragm, originates from the cervical spine at levels C3, C4, and C5. These are the exact same spinal levels that supply nerve signals to your shoulders and arms.
This shared neurological pathway is the anatomical reason why diaphragm and shoulder pain so frequently occur together. When the diaphragm is not functioning efficiently, the brain can misinterpret the neurological signals and register the discomfort as referred pain in the shoulder region. Countless people have undergone shoulder surgery or years of physical therapy without improvement — simply because no one investigated the diaphragm.
Understanding diaphragm and shoulder pain from this anatomical perspective completely changes how we approach treatment. The shoulder is not the source. It is the messenger.
How Diaphragmatic Dysfunction Creates Chronic Shoulder Tension
When the diaphragm weakens or loses its proper movement pattern, the body does not stop breathing. Instead, it recruits secondary muscles to compensate — specifically the scalenes, the sternocleidomastoid, and the upper trapezius. These are muscles located in your neck and upper shoulder region.
Every single breath then becomes a micro-contraction of your shoulder muscles. Multiply that by 20,000 breaths per day, and you begin to understand why diaphragm and shoulder pain creates such persistent, treatment-resistant tension. The shoulder muscles are being overworked not from exercise or injury — but from the simple act of breathing incorrectly around the clock.
I see this pattern clearly in desk workers, drivers, teachers, and caregivers — anyone who holds a fixed posture for long hours. Chronic stress compounds the problem significantly. Under stress, breathing becomes shallower and faster, accelerating the recruitment of shoulder muscles and deepening the diaphragm and shoulder pain cycle.
What I Observe Before I Touch the Shoulder
In my 12 years of clinical experience at Haim Body Balance Center, I have developed a specific observation protocol before I address any shoulder complaint. I watch the breath first.
Does the chest rise while the abdomen remains flat? That is an immediate red flag for diaphragm and shoulder pain. Does the client sigh frequently, hold their breath under mild stress, or struggle to breathe deeply on command? Each of these patterns tells me the diaphragm is not functioning as the primary breathing muscle.
One client — a 52-year-old teacher — had lived with left shoulder stiffness for two full years. X-rays were clear. MRI results showed minimal findings. Three separate clinics had treated her shoulder directly with zero lasting improvement. When I observed her breathing pattern, the answer became obvious immediately. She was breathing in a shallow, chest-dominant pattern that had been recruiting her left upper trapezius with every single breath for years.

This is the hidden reality of diaphragm and shoulder pain that conventional treatment consistently misses.
The Unconscious Nerve Brake: Why the Body Gets Stuck
Here is what makes diaphragm and shoulder pain particularly difficult to resolve with standard treatment. The problem is not simply muscular. Over time, as the body adapts to dysfunctional breathing patterns, the unconscious nervous system begins to lock the tension in place.
I apply the Kim Se-yeon Sbonsdo Unconscious Nerve Management method — a specialized technique that uses a 0.3-second stimulus to release the unconscious nerve brake. This is the key distinction between temporary relief and genuine recovery. When the unconscious nervous system has been holding a tension pattern for months or years, no amount of conscious stretching or exercise can fully override it. The brake must be released at the neurological level first.
With the 52-year-old teacher I mentioned, I applied this unconscious nerve brake release before addressing her breathing or her shoulder directly. Within three sessions, the shoulder stiffness she had carried for two years began to dissolve. She told me it was the first time any treatment had produced a result that actually held.
This neurological release is the foundation of how I approach diaphragm and shoulder pain — not from the outside in, but from the nervous system outward.
The Recovery Sequence That Produces Lasting Results
Once the unconscious nerve brake has been released, the body becomes ready to receive the following recovery steps. Attempting these without the neurological preparation produces only partial results.
Step 1: Unconscious Nerve Brake Release
This is the non-negotiable first step in resolving diaphragm and shoulder pain at the root level. The 0.3-second stimulus of the Sbonsdo method signals the unconscious nervous system to release its protective tension lock. Without this step, the muscles will return to their habitual holding pattern regardless of what other interventions are applied.
Step 2: Diaphragmatic Breathing Retraining

listen to our 432Hz healing music:
Lie flat on your back. Place one hand on your chest and one hand on your abdomen. Focus on breathing so that only the lower hand rises. The chest should remain relatively still. Practice this for ten minutes daily. This simple exercise begins to break the diaphragm and shoulder pain feedback loop by restoring the diaphragm to its role as the primary breathing muscle.
For more information on diaphragmatic breathing,
visit Mayo Clinic.
Step 3: Crocodile Breath Training
Lie face down on the floor. With each inhale, focus on feeling your lower back and ribs expand outward. This position trains the diaphragm to work against gravity, building endurance and depth that most people have never developed. Clients who practice this consistently report significant reduction in upper shoulder tension within two to three weeks.
Step 4: Thoracic Spine Mobility
A stiff thoracic spine mechanically restricts diaphragm movement. When the upper back cannot move freely, the diaphragm cannot fully descend during inhalation. Opening thoracic mobility gives the diaphragm the space it needs — and when the diaphragm moves freely, the shoulders no longer need to compensate. This is one of the most direct ways to interrupt the diaphragm and shoulder pain cycle structurally.
Step 5: Psoas Release
The diaphragm and the psoas muscle share fascial connections through the anterior spine. Releasing the psoas consistently produces immediate relief in both the core and the shoulder girdle — a result that surprises almost every client the first time they experience it. Addressing the psoas is an essential but frequently overlooked component of resolving diaphragm and shoulder pain comprehensively.
Identifying Your Own Risk Pattern
Not everyone experiences diaphragm and shoulder pain the same way. Here are the self-assessment signs I ask every new client to reflect on before their first session.
Do you breathe primarily from your chest rather than your belly? Do you find yourself holding your breath during concentration, stress, or physical effort? Do you sigh frequently throughout the day? Does your shoulder tension return rapidly after massage or stretching? Have you received multiple rounds of shoulder treatment without sustained improvement?
If you answered yes to two or more of these questions, there is a significant probability that diaphragm and shoulder pain is the underlying pattern driving your symptoms. The shoulder is not the origin. The breath is.
Long-Term Prevention: What Every Client Needs to Hear
Resolving diaphragm and shoulder pain is not achieved through a single treatment or a short course of exercises. It requires a fundamental shift in body awareness — specifically, the habit of monitoring your breathing during ordinary daily activities.
Not at the gym. Not during yoga class. At your desk, in your car, while preparing a meal, while talking on the phone. These are the moments when dysfunctional breathing patterns operate without your awareness. These are the moments that determine whether your shoulder tension will return or remain resolved.
When the diaphragm moves freely and the unconscious nerve brake has been released, the shoulders follow naturally. The body does not need to be forced into alignment. It finds its own balance when the root cause has been genuinely addressed.
After 12 years of working with clients whose diaphragm and shoulder pain had been misdiagnosed, undertreated, or dismissed entirely, the most consistent finding I can share is this: the breath is always involved. Always.
Start there. Everything else follows.
Disclaimer: This article is intended for general informational purposes regarding diaphragm and shoulder pain. If you are experiencing severe or persistent shoulder pain, please consult a qualified healthcare professional for personalized evaluation and treatment.
If you are also experiencing chronic pain beyond
the shoulder, read our guide on
How to Fix Chronic Pain: 5 Hidden Signs in Your Body to understand how foot alignment and body
imbalance connect to your daily pain patterns.
How to Stop Plantar Fasciitis in 4 SessionsHow to Stop Plantar Fasciitis in 4 Sessions